Summary
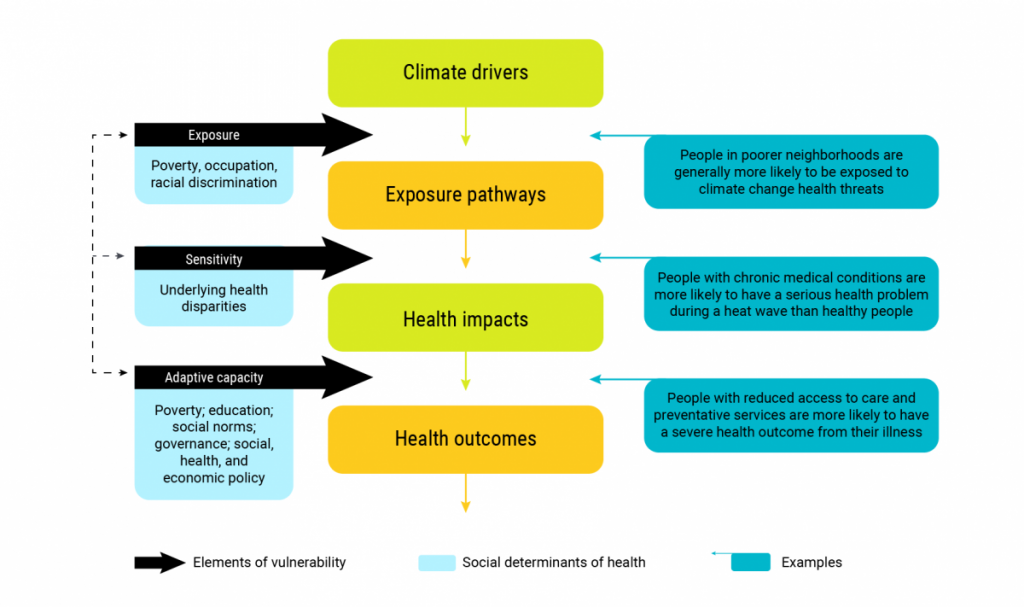
Changes in climate are exacerbating existing health inequities and creating conditions for new inequities to emerge. The health effects associated with climate change will not be experienced uniformly. Vulnerability to health impacts of climate change is determined by the exposure to climate change hazards, the sensitivity to possible impacts, and the capacity to respond to, or cope with them. At the individual level, these three factors are influenced by determinants of health, such as socio-economic status, housing quality, and education. Determinants of health interact and intersect with inequities in complex ways that render the experiences of diverse groups and individuals unique. Structural systems of oppression, such as racism and colonialism, also influence an individual’s vulnerability to climate-related health risks. Therefore, effective adaptation measures must be intersectional and equity-based. If adaptation efforts are not carefully planned, adaptation efforts may benefit only part of the population, and inadvertently worsen existing inequities. Resilience and asset mapping, vulnerability mapping, equity impact assessments, and meaningful and inclusive community engagement and communications can all contribute to equity-centred adaptation measures.
Key Messages
- Climate change can exacerbate existing health inequities, defined as avoidable and unjust differences in health. These inequities — for example, disproportionate impacts on health from extreme heat — can increase the health risks from climate change for some individuals and populations. Knowledge gaps and data limitations make it difficult to assess and measure how climate change has already affected, and will continue to affect, health equity in Canada.
- The pathways through which climate change affects health inequities are complex and dynamic. These pathways often involve the conditions and factors that affect a person’s health, known as determinants of health (such as, income, education, employment, and working and living conditions), which can increase or decrease an individual’s exposure or sensitivity to climate-related health hazards and can create barriers that limit their ability to take protective measures.
- Structural systems of oppression (such as, racism, heteronormativity, and ableism) that result in health inequities are underlying drivers of vulnerability to climate change.
- Health equity should be an important focus of climate change and health vulnerability and adaptation assessments and related knowledge development activities. Mapping tools (asset mapping, vulnerability mapping), enhanced data collection, and inclusive community engagement will help identify populations and regions at increased risk, and better inform adaptation measures.
- Climate change adaptation measures meant to protect human health are not experienced in the same way across populations and communities. In the absence of careful planning, adaptation efforts may benefit only part of the population and inadvertently worsen existing health inequities.
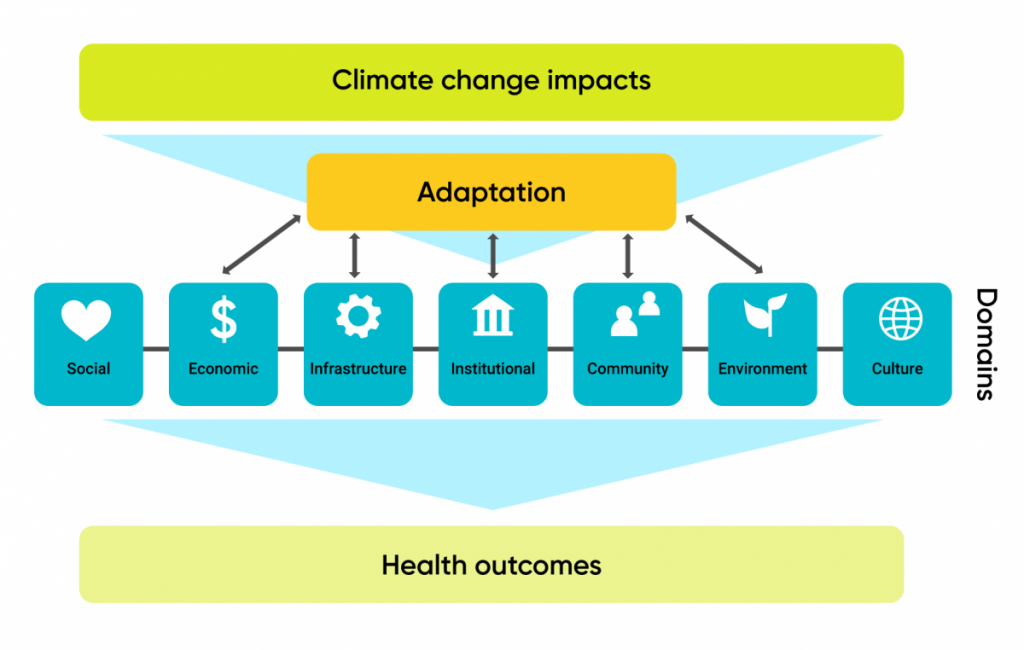
- Health equity can be increased and determinants of good health strengthened through adaptation. Public health authorities should ensure that adaptation measures are planned and implemented so that people who are disproportionately affected by a warming climate benefit from them.
- Ensuring inclusive, equitable, and community-based participation in the adaptation process is critical for designing and implementing effective adaptation actions that protect the health of all Canadians. Participation of racialized and marginalized individuals and communities that already experience a disproportionate burden of illness and health inequities is required.
- Climate change mitigation and adaptation measures implemented outside of the health sector may affect determinants of health and health outcomes, in either positive or negative ways. Public health authorities can ensure that climate action supports health equity and related positive health outcomes in Canada through collaboration across jurisdictions, sectors, and disciplines.
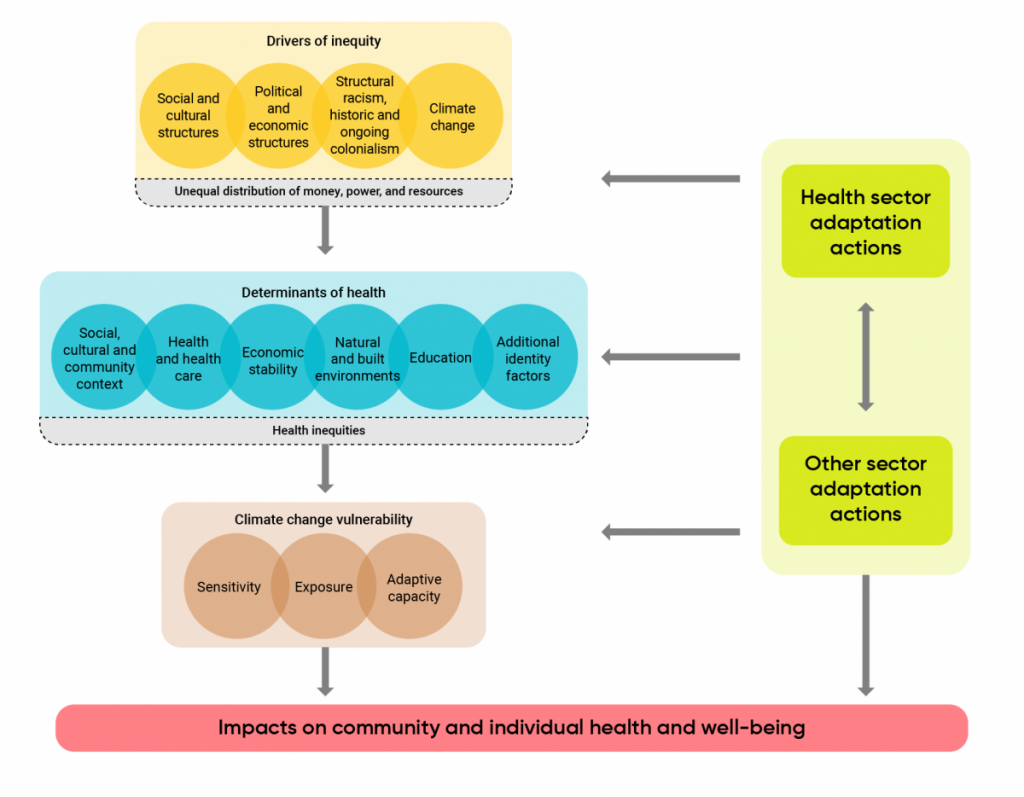
Figure 9.1
Climate change and health equity framework.